BMT-01.10 Executive Summary#
BlueMirror.tech | May 2026#
Margaret’s daughter, on a recent visit to Sacramento, opened her mother’s refrigerator and recognized very little in it. The dietary changes had not been announced. They had emerged across nine months: more fish, less red meat, a shift to whole grains, the disappearance of canned soups, the appearance of low-sodium versions of items Margaret had bought in their familiar versions for forty years. The daughter recognized the result as the cardiologist’s recommendations finally being followed. She did not know how. Margaret had never managed her diet by rule. She cooked what she liked from what was in the kitchen. Yet what was in the kitchen had changed.
The nutrition concierge is what changed the kitchen, not by issuing instructions Margaret would have to follow, but by coordinating with the buying agent that purchases the groceries, with the health concierge that holds the dietary restrictions, with the cognitive concierge that knows what mental load is reasonable on a given day, and with the social concierge that recognizes meals as social acts. The result is that what arrives in the kitchen is consistent with the dietary guidance, while what Margaret cooks remains hers. Nutrition spans health, buying, culture, preference, and social eating, which is why it is a separate concierge agent rather than a feature of the health concierge.
The naïve architecture would make nutrition a function of the health concierge, since the health concierge holds the dietary restrictions and dietary intake affects health outcomes. The argument fails on closer inspection. The health concierge’s frame is clinical: medication, vital signs, symptoms, appointments, transitions between care settings. Nutrition fits poorly because most of nutrition is not clinical. Most is cultural, social, economic, and pleasurable. Margaret’s Wednesday cooking class with the student in Brisbane is a nutrition event. So is her grocery list, her decision to invite a neighbor for dinner, her management of her budget, her cultural preference for ingredients she grew up with, her grandson’s allergy, her cognitive capacity to plan three days of meals on a Sunday afternoon. None of this is clinical. All of it is nutrition. The reverse architecture, nutrition as a feature of health, would either neglect the non-clinical dimensions or smuggle non-clinical concerns into a frame not designed for them. The architectural lesson generalizes: decomposition follows the contour of the user’s life, not the contour of the technical capabilities that compose to serve it.
The nutrition concierge composes from one primary infrastructure agent (the Nutrition Tracker, 0.5 autonomy, edge deployment) plus shared services. The Nutrition Tracker maintains the structured nutrition context: dietary restrictions and their sources, cultural and personal food preferences, cooking ability and energy patterns, and intake patterns over time. The Nutrition Analyst SLM runs at 100M parameters and targets under 75ms inference. Its job is to compose meal plans against the constraint set, generate recipe suggestions, evaluate substitutions for dietary compliance, and answer questions Margaret asks about nutrition. The model is deliberately small because most nutrition reasoning is structured: lookups against ingredient databases, application of rule-based dietary constraints, simple optimization across a constrained menu. The complex reasoning happens elsewhere. This pattern of parsimonious parameter sizing repeats across the system. Edge feasibility is a design constraint, not an aspiration.
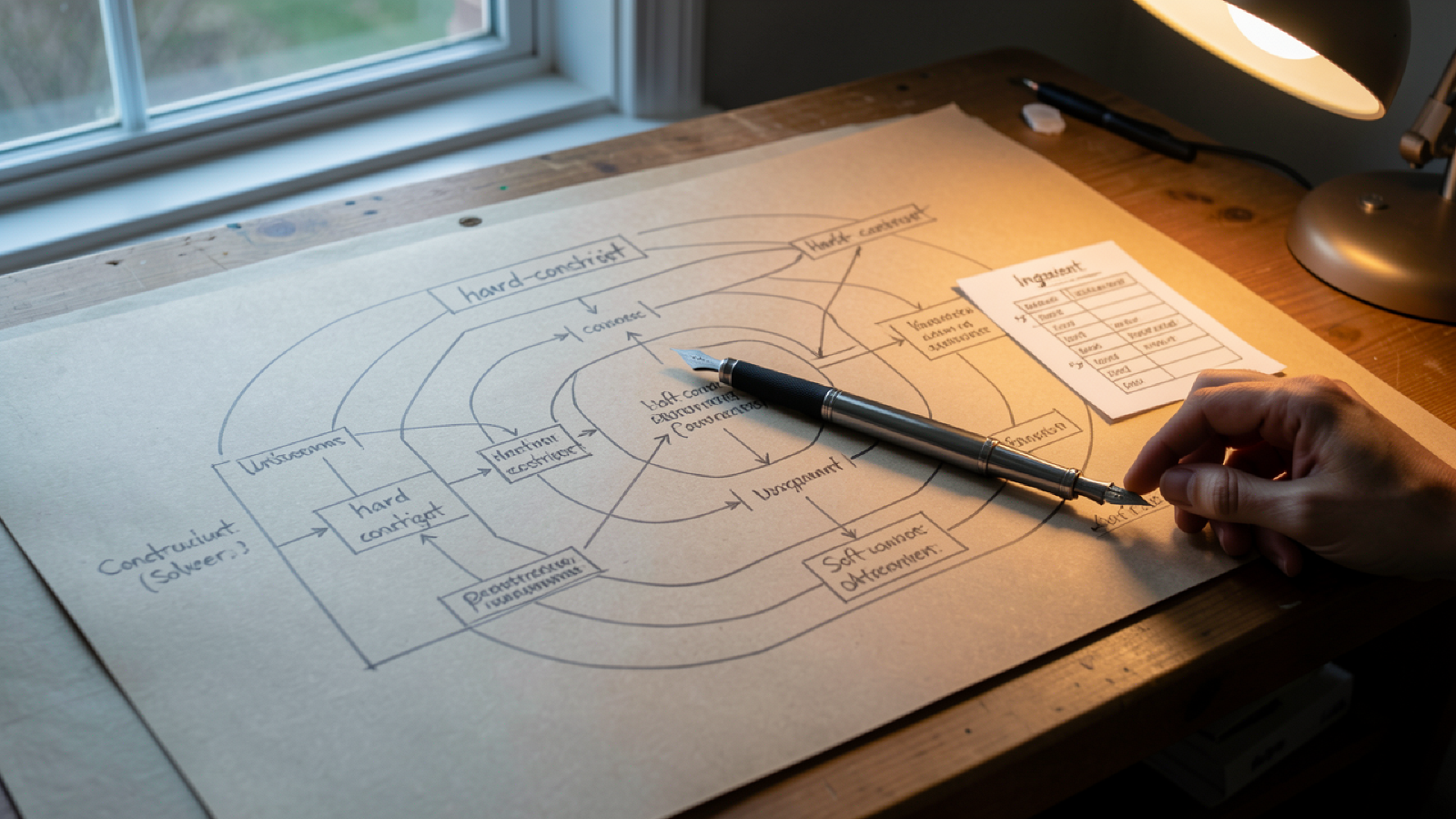
The cardiologist updated Margaret’s sodium restriction from 2,000 mg/day to 1,500 mg/day on a Tuesday. By Tuesday evening, the nutrition concierge had updated the meal plan, the buying agent had adjusted the grocery list, and the family coordination concierge had updated the daughter’s view of the household nutrition picture (with Margaret’s consent, configured to share dietary changes without sharing the reason). The integration is the architecture in one example. The dietary update did not require Margaret to do anything. The cardiologist wrote it into the FHIR record. The health concierge propagated the constraint to the nutrition concierge. The nutrition concierge ran its constraint solver against the existing meal plan and produced an updated plan that maintained Margaret’s preferences and cultural patterns while reducing sodium to the new target. The buying agent received the updated plan and adjusted the grocery list.
The constraint solver is structurally interesting. Margaret’s dietary constraints are partial, weighted, and sometimes contradictory. Hard constraints are non-negotiable: no shellfish, no MAOI-incompatible foods. Soft constraints are weighted: low sodium (clinical, recently changed), low added sugar, high fiber, affordable, culturally meaningful, familiar (weighted lower on most days but higher on cognitive low-capacity days), prepared from ingredients she enjoys cooking with. The solver does not produce one optimal meal plan; it produces a feasible plan that respects hard constraints and surfaces tradeoffs when the constraint set becomes infeasible. When the new sodium restriction made several of Margaret’s longstanding favorite dishes infeasible at the previous preparation, the solver did not silently remove them. It surfaced the tradeoff: the chicken cacciatore at 1,400 mg of sodium per serving could be modified to 750 mg with reduced-sodium broth and tomato paste, with some change in flavor. Margaret tried the modified version. It worked. The dish stayed in rotation.
Cultural food preferences are the agent’s most underdeveloped capability today and one of its most important. Most nutrition guidance in the United States is built against an implicitly Anglo-American baseline. The dietary advice that works for a person whose meals revolve around bread, salad, and grilled protein does not translate cleanly to a person whose meals revolve around rice, beans, and stewed vegetables, or dumplings and congee, or couscous and harissa. The agent maintains a structured representation of cultural food context: regional traditions, family recipes, ingredient preferences, religious or ethical eating patterns. The constraint solver respects these as soft constraints with high weights. The architecture’s job is not to convert Margaret’s eating into something the model thinks is healthier; it is to support her in eating well within her own tradition. The honest limitation is uneven cultural coverage; the system has good representation of major U.S. immigrant traditions where the user population produces a meaningful training signal and weaker coverage of smaller diaspora communities. The agent’s response in those cases is to defer to the person’s expressed preferences rather than impose a model-derived assumption.
Meal planning as cognitive support is a pattern that emerges across users with mild cognitive change. The structured rhythm of meal planning, grocery shopping, and cooking is itself a cognitive scaffold. The person who knows that Tuesday is fish night, Wednesday is pasta, Thursday is the farmers’ market has a structure that supports executive function. The agent supports this rhythm without imposing it. Grocery integration with the buying agent runs through shared context rather than API calls. The meal plan is in the shared context; the buying agent reads it on its scheduling cycle and adjusts the grocery list. The integration handles edge cases: unavailable ingredients trigger substitution discussion before order; price spikes trigger recipe alternatives; visitors trigger quantity adjustments.
For the full treatment of why nutrition is its own concierge, the constraint solver, cultural preferences, and the buying-agent integration, read the complete article on BlueMirror.tech.